Categories
Speciality Areas
Mattress Flammability Risks: What Medical Device Testing Needs to Consider

Flammability testing of mattresses tends to be based on furnishings flammability testing, but are these fit for purpose for medical devices, with their varying designs and structures?
Where issued on a bed for the prevention or alleviation of skin pressure injuries, the mattresses provided will be medical devices as specified by their manufacturer. For the protection of the patient and carers, the risk of harm from ignition of the materials used should be minimised, but not at the cost of increased risk of tissue damage. But how much of the risk comes from the medical device, and how much from human behaviour and other external factors?
Human Factors
This topic was highlighted in a recent Society of Tissue Viability webinar1 which concentrated on the challenges presented by “air powered” mattresses where if punctured by an ignition source, the air pumps increase the airflow, thereby “fanning” the flames. Dr Jeannie Donnelly (Lead Nurse – Tissue Viability, BHSCT (Belfast Health & Social Care Trust)) presented a case study which highlighted all the risks to and from a specific individual, who was a smoker. She emphasises the needs to:
- Recognise human factors which must be considered prior to providing a powered mattress to people who smoke.
- Discuss potential intervention strategies and their effectiveness in minimising the risks associated with accidental dwelling fires.
- Examine the role of individuals, and agencies, that are in contact with people at risk and how they can be employed to reduce the risk from fire.

Peter Cassidy, Station Commander with the Northern Ireland Fire and Rescue Service, describes the Safer Together project they have carried out with BHSCT to try to reduce the risks from fire for the Trust’s patients. Part of this was to produce an e-learning package2, of value to anyone who may be in contact with a “vulnerable” patient. This includes a Risk Awareness Form listing Red Flag Indicators to be brought into the total risk assessment process, as well as other useful items such as posters. The project has just won the Regional Social Care Award 2025!
Elements of Human Behaviour (2020-2022)
Elements of human behaviour in the 32 fatalities recorded between 2020 and 2022 were highlighted by Peter:
- 94% were people over the age of 50
- 44% were triggered by smoking
- 53% of the individuals were known to the services
- 30% were discovered by carers
Procurement
In prescribing a suitable pressure care product, where does one start? From a procurement perspective, what should be specified within the description of the relevant flammability criteria for selection of a pressure care device? The answer is that there is no simple answer, and it all falls back on the assessment of “risk”. Even that is not straightforward since often we have a range of external risks, such as the behavioural aspects outlined above, that are external to the device being specified. Each sits at a point somewhere along a risk scale. It is the summation of the external risks relating to fire that will guide the degree to which the pressure care device needs to manage the fire risk. The end result inevitably will be some kind of compromise.
For this article, we concentrate on pressure care devices which are offered as “medical devices” since these are specifically excluded from UK fire regulations, whereas domestic beds, mattresses, and cushions fall under furnishings fire regulations.
Environmental Inputs
The following are some of the inputs needing to be considered for the risk assessment. These cover the environmental risks to a patient. Once these have been assessed, the properties of the pressure care device itself will come into play.
Use Environment
The scale of risk from fire will vary, depending on where the patient is situated. This will be along the scale of increasing risk from hospital to residential home to domestic home to “institutions”, such as prisons.
In the US, this is managed by requirements that institutional, i.e. non-domestic, settings have sprinkler systems to manage any fire, rather than relying on the pressure care device to control the fire risk. Note that in England new-build residential homes must now have sprinkler systems installed.

User – Mobility
In the case of fire, how easily can the individual get away from the conflagration? If the user has impaired mobility, then the flame retardancy of the pressure care device becomes more important.
User – Behaviour
There are environments where the degree of risk from the patients’ behaviours, be it from smoking, mental stability, cognitive ability, disruptive arson, or other, need to be taken into consideration.
User – Extraneous Risks
Is the patient on oxygen and therefore potentially offering up a greater risk if a small fire were to start? Is the patient being treated with emollients?3 These are usually made up in volatile flammable solvents, and can be on the patient’s skin, on their clothing, and/or on their bedding.
Emollients have been shown to be a much higher contributor to patient burn injuries than previously thought. How flammable are their clothing or their bed coverings in their own rights? Are alcohol wipes being used? There are many examples of cautery devices setting light to drapes in operating theatres.

User – Pressure Care Device Application
There will be less fire risk around a small device such as a wheelchair cushion than a full-size mattress, for example. When selecting a cushion for a wheelchair the risk from fire has been shown statistically to be very low, in part because the occupant’s body covers most of the pressure care product, whereas the potential risk of skin damage is higher, because of the higher forces and lengths of time involved.
Product Elements
As the environmental risk score increases, the prescriber needs to compromise increasingly between the risks to the patient from the environmental factors versus the risk of the “fire-proof” materials to their skin health. If the combination of all the environmental risks is low, or manageable, then full attention can be turned to the patient’s risks of tissue injury, and how to prevent it.
User – Medical
The leading question here is which is the greater risk to the patient: serious health impairment from tissue injury or from fire.
Ignition Resistance vs Retardancy
Around the world, most of the flammability standards have had as a minimum a lighted cigarette test and a flame test. In the UK we have also had Crib tests where increasing amounts of heat have been applied to the device: a Crib 5 test is a heat source designed to burn for five minutes, and a Crib 7 test for seven minutes, for example.
Two aspects are of relevance from the testing: how easily will the device catch light, and if, once alight, how quickly will it self-extinguish.
Fire Retardants
Various fire retarding additives have been banned around the world arising from concerns about their biocompatibility when coming into contact with naked skin. For cover materials that are washed or cleaned down, do the retardants get washed away or deactivated – so should the device be tested as new or after a number of wash cycles? Fire retardants in foam decrease their useful life, but may be needed for the foam to pass flammability tests.
Materials
Should the cover on its own and the inner material on its own be tested individually and/or as a composite? Even if the material passes the flammability self-extinguishing testing, what is the risk of hydrocyanides and other gases given off while the product was combusting?
Where Are We Going?
While furniture flammability tests are the current basis for testing medical support surfaces in many parts of the world, these tests will be heavily weighted around furnishings being made with polyurethane foam fillings, and the fire source coming from above.
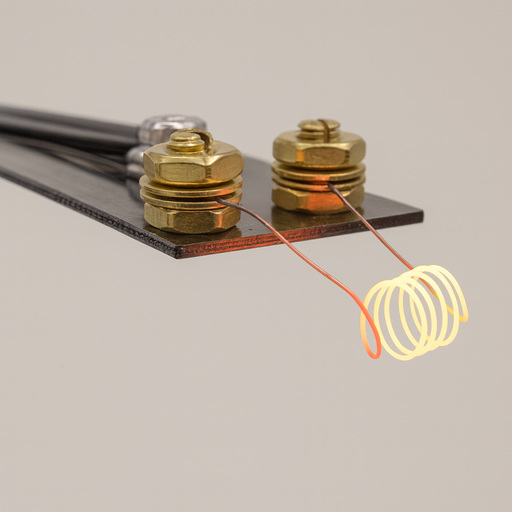
The international wheelchair cushions standards working group came to the conclusion that a cigarette type of test would be appropriate around all the external and medical risks. They found that there was no such thing as a standard cigarette, however, so they came up with a surrogate cigarette in the form of a NiCr coil through which a suitable current is passed, and this has been accepted around the world including by the FDA: The standard is ISO 16840-10 plus Amd14. This test method is suitable to be used equally with foam filled, gel filled, air filled, or air-powered products. It also addresses testing all surfaces, top, side, or bottom, that might be at risk.
This is being investigated by the international mattress standards working group and the US Consumer Product Safety Commission as being appropriate for mattresses. The coil current can be turned up to give the equivalent heat output of a flame or a Crib test. Meanwhile the furnishing cigarette, flame, and Crib tests will continue to be called up, until an alternative is agreed upon.
Finally: Returning to the case study referred to at the start of this article, where the patient presents a high risk from his smoking habits, I would avoid prescribing an air-powered pressure care mattress, since there is still a good range of alternative pressure care devices suitable for patients at high risk of tissue injury. If we compare the prescription of air-powered devices in the UK with the rest of the world, dare I ask if they are over-prescribed?
References
- https://www.youtube.com/watch?v=SbN9URbm4dE
- https://rise.articulate.com/share/Paw_3tCeSK4-e2ViBd5Qc7SLSMu525O6
- Ridd, M. J., Hall, S., Lane, M.E., Roberts, A., and Williams, H.C. Burns with emollients. The British Medical Journal, practice – adverse drug reactions, 2022, 376. https://doi.org/10.1136/bmj-2021-066102
- ISO 16840-10:2021 + Amd1:2024 Wheelchair seating – Part 10: Resistance to ignition of postural support devices – Requirements and test method.