Categories
Speciality Areas
Slip Sliding Away

When someone slips down in their seat or chair, why do they do it? Is it a bad thing? Why do we try to stop it?
As children we were probably at meals, or even school, told to sit still and sit up straight! Why were we told this? For meals it’s a practical thing in that we are less likely to spill food down our fronts. At school, it can indicate the pupil is alert, interested, and paying attention: however, because of the muscles involved in sitting up, this can involve more energy than if slumped in our seat. Slumped shoulders can also give an indication of a person’s psychological state. However, when we want to relax and overcome postural fatigue, most of us go into a posterior pelvic tilt, and let our backs sink into the back of our seating. Why might this be a bad thing? We all want to relax at some time during the day, surely?
A Bad Thing?
This is a bad thing if we are unable to change our position for ourselves to get back to an alternative position. This is a bad thing if it means that, as a result of slipping down, our secondary support devices risk strangulating us. This is a bad thing if the accompanying friction around the buttocks, and the shear stresses and strains involved, risk damage to skin tissue. This is a bad thing if it leads to the longer term development of a kyphotic curvature of the spine. This is a bad thing if the kyphotic posture means that it is hard to see in front of us without having to hyperextend the neck. It is a bad thing if the kyphotic posture leads to drooling. This may also be a bad thing if the result is that your head ends up being lower than it could be, thereby limiting your ability to look over an obstacle, or look someone in the eye.
Why Does It Happen?
Surprisingly, a common cause of our posterior pelvic tilt can be the position of our feet! Many people, in care homes for example, are left in transit wheelchairs for much of the day. These chairs often have their foot supports positioned well in front of the chair casters to avoid the foot supports interfering with the casters’ movement. Unfortunately, many of these occupants also have shortened hamstrings. These hamstrings that attach to the top of the lower leg at one end, attach to the base of the pelvis at the other. The consequence of having the feet pushed out in front of the chair is that the lower leg is stretched forward, and this in turn pulls, via the shortened hamstring, on the pelvis, pulling the occupant’s pelvis forward, and at the same time rotating the pelvis into a posterior tilt.
If the chair’s seat depth is too long, this too can lead to the pelvis not being able to connect with the back support, and the occupant slips into a posterior pelvic tilt and with a kyphotic spine to accommodate this space.
From another angle, a set or fixed kyphotic curvature of the spine is usually associated with a compensatory posterior pelvic tilt. And as indicated above, the consequent posterior tilt can lead to sliding out of the seat.
What Can We Do About It?
Let’s start by fitting the chair correctly to the occupant and their range of movement. Make sure the effective seat depth is no greater than the occupant’s thigh length. Make sure that the foot supports on the chair are positioned sufficiently far back so that the occupant’s hamstrings are not forced to pull the occupant’s pelvis forward.
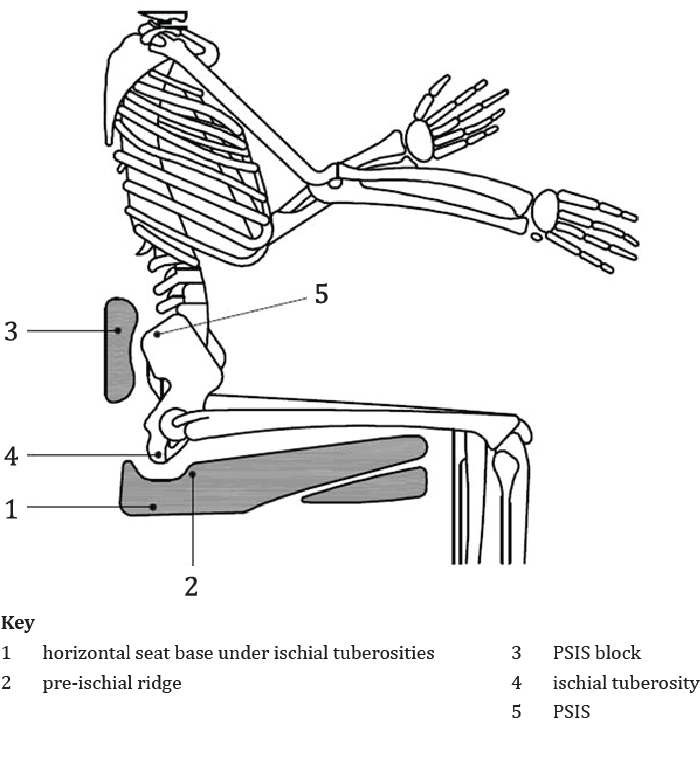
If we were to treat the pelvis as if it were a ball, and that you wanted to stop it from rotating and rolling away (since this is in effect what is happening), what would be the best means to achieve this? First, to stop it rolling backwards, place a block high up behind it: in effect behind the posterior superior iliac spines (PSIS) (4 and 6 in Fig. 1). Then to stop the ‘ball’ rolling forward, have a pre-ischial ridge in the seat cushion (2 in Fig. 1), just in front of the ischial tuberosities (ITs) (5 in Fig. 1). Note that this ridge does not need to be more than 5 mm in depth – anything more risks increasing anterior pressures on the ITs.
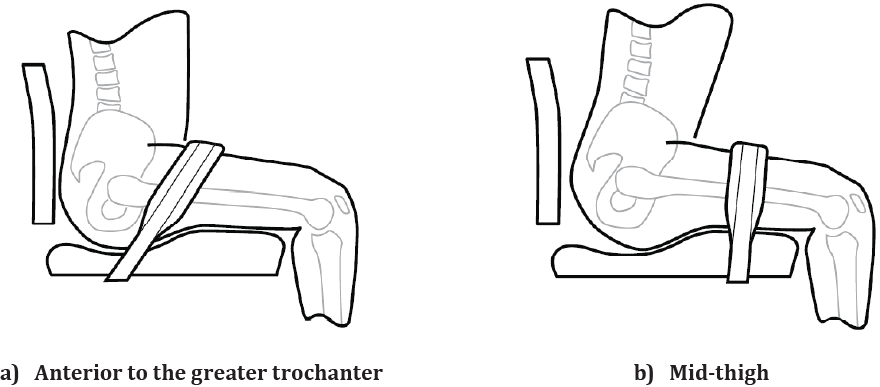
On the principle of three points of control, a pelvic positioning belt positioned across the thighs will assist further to keep the pelvis in place (Fig. 2).
An alternative can be leg harnesses (Fig. 3), which have the further advantage of giving separate control to either side of the pelvis. In contrast, the use of knee blocks to achieve this aim is generally deprecated due to the forces on the hip joint that these can induce.
Other aspects of the seat cushion can also have effects. Consider a cover material that can be ‘grippy’, especially under the thighs (though this does need to be balanced against the additional shear stresses and strains this can bring to the skin tissues, especially under the buttocks). Other aspects of the mix of materials internal to the cushion design, in addition to the pre-ischial ridge, can provide additional lateral and posterior supports, giving the benefit of helping position the pelvis more securely (for an example, see Fig. 4).

While considering the cushion, a wedge placed under the cushion under the thighs has been shown to be effective at redistributing pressures away from the buttocks, while still allowing the foot supports on the wheelchair to be positioned at a suitable height from the floor (3 in Fig. 1).
Moving Up the Body
We have linked a kyphotic posture of the back with a posterior pelvic tilt. Where the kyphosis has become ‘fixed’, this can be accommodated to some extent by opening up the angle of the back support. Remember that, for a standard back support (without biangular or multiangular aspects to its design), the bottom of the back support is ideally placed as a PSIS block to control the tendency towards a posterior pelvic tilt as much as is feasible (and comfortable), but still allows the back support to be angled back to accommodate the needs of the thoracic region of the occupant’s torso, be it the kyphotic region of the spine, or the shoulder blades.
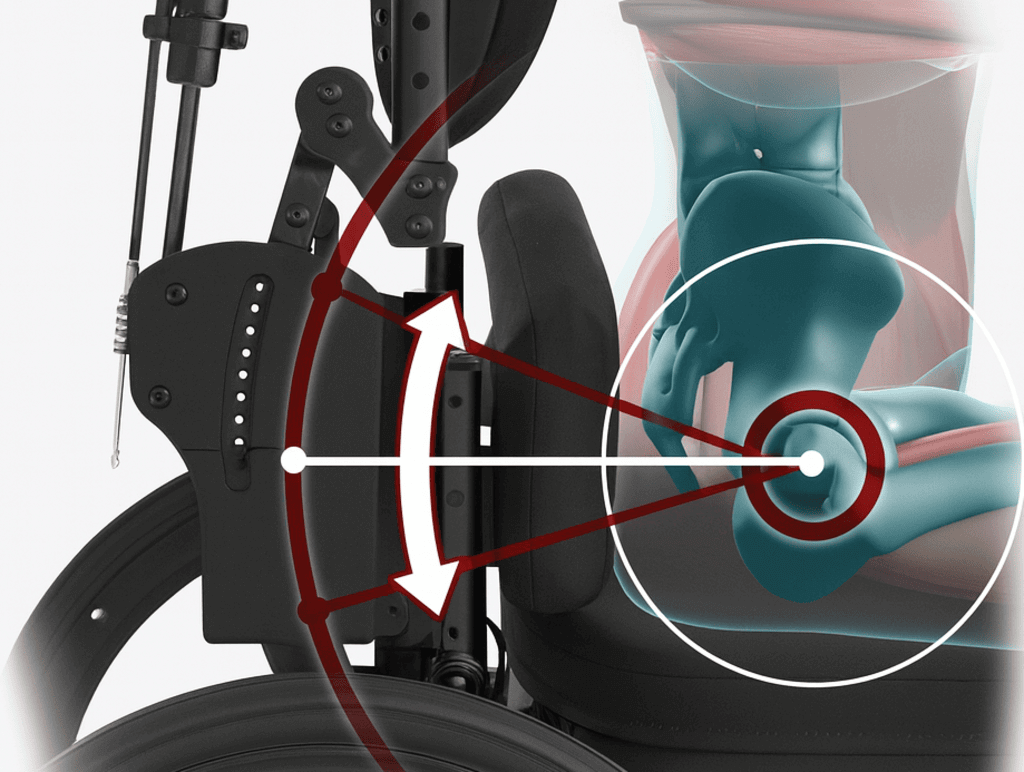
If a variable recline position is offered as part of the wheelchair design, please do make sure that the recline pivot point is level with the occupant’s hip joint (for example, as in the EPiC seating system – Fig. 5), rather than pivoting below this at the back support-seat base junction. Meeting this requirement again allows the pelvis to remain in a neutral position, while allowing the postural variation of reclining the back support for relaxation, for example, and without creating shear forces along the occupant’s back.
In Conclusion
To help the seated occupant from slipping down in their seat, it’s best to help them to maintain as neutral (i.e. vertical) a pelvic position as possible. This can be achieved by a mix of wheelchair set-up from the feet, through the seat base, to the back support. Alongside this, the placement, design, and materials, of the seat cushion and other postural supports will be important.
References
- BS ISO/TS 16840-15:2024 Wheelchair seating — Part 15: Selection, placement and fixation of flexible postural support devices in seating