Categories
Speciality Areas
Child or Adult? What’s the Difference?

When we are assessing, procuring, supplying, or fitting equipment, what are the implications around so-called ‘paediatric’ equipment? Where do we take aboard legal ages versus chronological ages, mental ages, or physical development? Where might it be more appropriate to issue ‘adult’ equipment to a child, and when might it be appropriate to issue ‘paediatric equipment’ to an adult?
When selecting equipment to prescribe to a user, which criteria are used by the manufacturer to guide us to the appropriate part of their catalogue? Often we see use of the terms paediatric or children, but does that actually point us in the right direction, particularly around the prescription of Assistive Products? These terms are usually associated with a chronological age, but is physical size more relevant? Or is the person’s ‘mental age’ going to be more relevant? In this article we look at the implications of these different aspects when choosing the relevant equipment for a specific individual.
Chronological age is a common measure since legislation is built around it. This governs the ‘age of majority’, currently our 18th birthday in the UK, at which point in the eyes of the law a person ceases to be a child.
So what age are you? Around the world most people follow the Gregorian calendar, based on the given date of the birth of Christ, and where 1 January is New Year’s Day. Our date of birth, and therefore our age, is based on our birth day on this calendar. (However, this is not necessarily the same all over the world – see box.)
However, when you reach 16 the law does actually start to move you over to adult status, both on the health and on the social services front1. From this age, you can consent to surgical, medical, or dental treatment, including the taking of blood samples. You can also choose your own doctor. You start to have to pay prescription charges (unless you are in full-time education, pregnant, receiving income support, on a low income, or in certain other circumstances). You start to have to pay for a sight test and for glasses (unless you are in full-time education). Etc.
Did you know?
In Japan, the current era and year relate to the date when the current Emperor ascended the throne, and at the time of writing is Reiwa 4 with each year starting on 1 May in the Gregorian calendar.
In China you can have two birthdays, one from the Gregorian calendar, and one from the Lunar calendar, which runs in 60 year cycles consisting of 12 lunar months and then a leap year of 13 months every three years. This year is 4720. In the lunar calendar you are 1 year old on your date of birth and you add one year on each new Lunar New Year’s Day. (In the UK we do something similar for racehorses whose birthdays are always 1 January).
If you are a ‘looked-after’ child, Children’s Services (formerly Social Services) have to give you support when you reach 16 and help you to prepare for leaving care. If you were ‘looked after’ by the local authority between the ages of 16 and 18, the local authority continues to be under a duty to advise and befriend you up to the age of 21. (If you are in higher education the local authority has a duty to assist you financially up until the age of 24 if necessary.) Part of this provision is to prepare a Pathway Plan, which should set out, inter alia, support for physical, emotional, and mental health needs. After the age of 21, however, you can get launched into a relatively unknown world.
From the medical point of view, paediatricians see patients up to the age of 18. Nonetheless, from the age of 16, patients are more likely to be cared for by ‘adult’ doctors, except in certain specialist cases. However, people aren’t considered fully grown until they turn 21, and the American Academy of Pediatrics recommends that patients should be seen by paediatricians through this age.
Our progression through childhood is broadly ascribed to different phases as follows, but with quite some variation: Neonates up to 1 month; Infants up to 2-4 years old; Children up to 11-14 years (i.e. puberty); Adolescents (or Youth) up to adulthood (which is treated, depending on the purpose, as anything between 16 and 25 years of age). For the supply of equipment to adolescents, there will be little difference in sizing from equipment designed for ‘adults’.
In Aristotle’s words: “Give me a child until he is 7, and I will give you the man”, and it’s during the period of development in the earlier years where we need to take most care as there is most change from day to day and week to week. This is very relevant to equipment provision where we need to facilitate the child’s maximum potential across the physical and mental spectrum – every week of delay is often a week that cannot be recovered later.
Mental age
While chronological age watches the clock tick by, what is happening to the human body as it ages through childhood? We have mental and physical development to contend with.
Mental age is a concept which tends to be linked to intelligence. This is measured by how a specific individual, at a specific age, performs intellectually, compared with average intellectual performance for that individual’s actual chronological age. The intellectual performance is based on performance in ‘intelligence’ tests. The test score achieved is compared with the median average scores for different ages, and the mental age is that for the nearest matching score. (A person’s IQ is derived from this mental age, divided by their chronological age, times 100).
Mental age on its own is not the complete picture. A person’s ‘mental age’ might be average for their chronological age, but the same person’s emotional intelligence might be immature (or advanced) for their chronological age.
Emotional intelligence (EI) refers to the ability to perceive, control, and evaluate emotions, and is most often defined as the ability to perceive, use, understand, manage, and handle emotions. Some researchers suggest that EI can be learned and strengthened, while others claim it is an inborn characteristic. During normal development, EI progresses through four stages: Self-awareness, Social consciousness, Self-care, and Relationship management.
Although an individual may have gone through the physical changes to adulthood, their mental age or emotional intelligence may be out of step, and this may be the more important aspect to consider when prescribing equipment.
Physical aspects
When providing Assistive Products, often we see equipment characterised as being ‘Children’s’ equipment, and this is probably because people are compartmentalised by their chronological age, with the background assumption that this will marry up with mental age, emotional age, and physical age, since most of these criteria are based around the ‘average’ person.
Across normal childhood, this approach can work reasonably well for many people up to the age of puberty, but soon after, as a result of rapidly increased body mass, muscle strength, etc there may be no difference in appropriate provision than for an average adult – and puberty can start at a wide range of ages.
The additional challenge for the clinician is that for a few years the rate of change, especially around puberty, is so rapid that the equipment may need to be adjusted or replaced every few months. There are also many smaller adults for whom ‘paediatric’ sized equipment might be more appropriate. (For children’s clothing, sizes that are designed to fit the average sized child up to the age of 14 are zero-rated for VAT, so the more petite or smaller adult can benefit from being able to wear these clothes.)
Equipment provision
So, can we move away from the concept of paediatric equipment, and accept that there is a continuum across chronological ages of physical size, physical dexterity, mental ability, emotional intelligence, as well as a spectrum of aesthetic perceptions, and categorise equipment by criteria that match a particular individual’s need?
In clothing, if you pick up a T-shirt sized M, this will be a different size depending on the country where it was made, and as a result for some people it will be very tight, and for others it will swamp them. We have seen the same challenge for wheelchair belts and harnesses. In BS 86252 (shortly to be published as well as ISO/TS 16840-15) this has been tackled by changing to equipment sizing based on the measures of the user – see Figure 1 and Table 1.
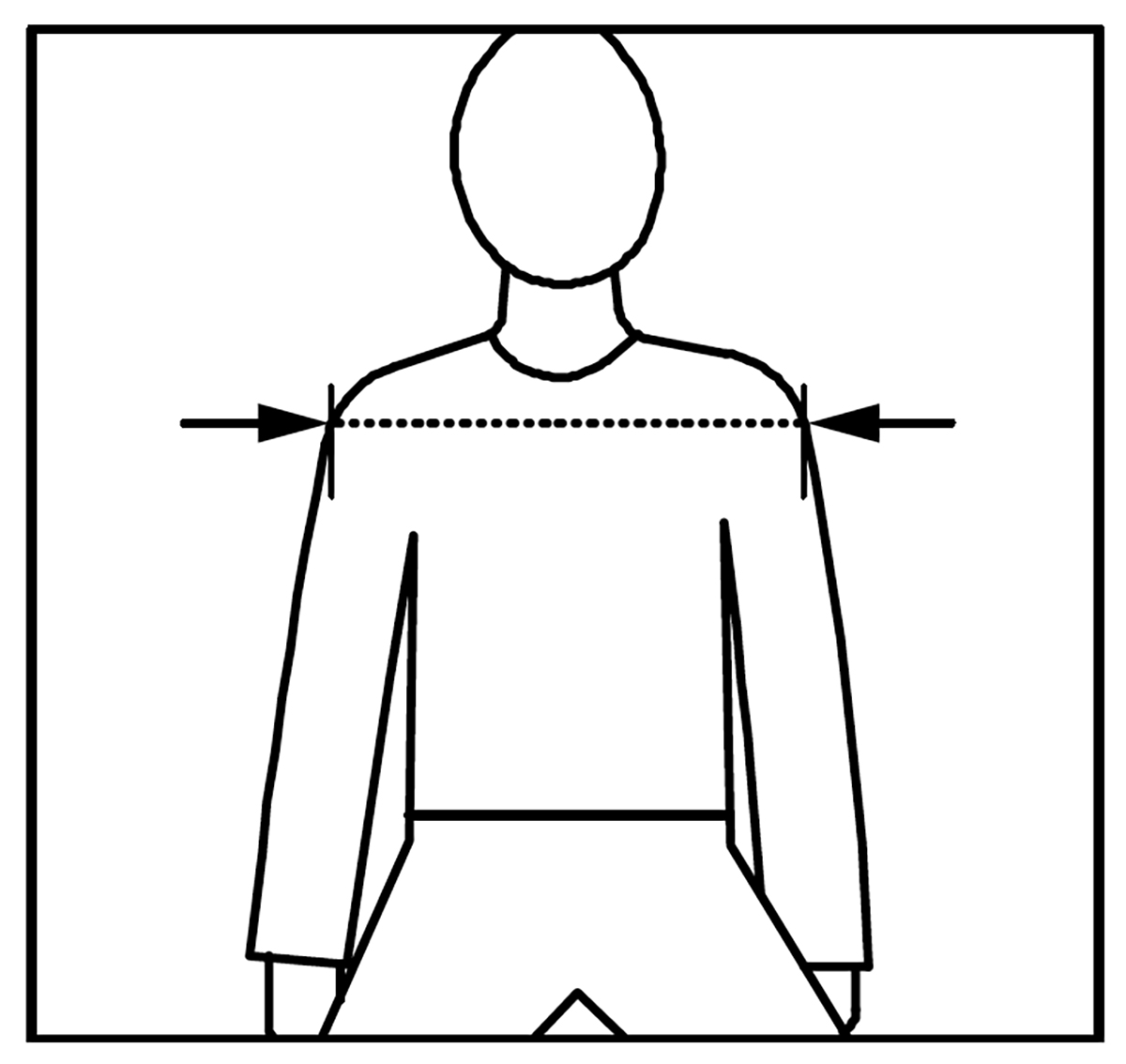
Figure 1 – Measurement for an anterior trunk support
This standard also addresses the type of closure system of a belt or harness that should be selected to suit the occupant’s and/or the carer’s ability to open the buckle, depending on their cognitive and/or physical dexterity, and this is not an age related matter.
| Anterior trunk support size | Designed for shoulder width (Fig 1) | Possibly previously described as |
| Size 15–24 | 150 mm to 240 mm | XX Small |
| Size 24–28 | 240 mm to 280 mm | X Small |
| Size 28–33 | 280 mm to 330 mm | Small |
| Size 33–41 | 330 mm to 410 mm | Medium |
| Size 41–48 | 410 mm to 480 mm | Large |
| Size 48–55 | 480 mm to 550 mm | X |
Table 1 – Anterior trunk support size selection
The approach to sizing shown in Table 1 means that each manufacturer has the option to make a device, in this case a shoulder or chest harness, to their choice of size range, and their smallest size might be a size 12-24 or a size 13-20 if they wished. The prescriber measures the client, and then picks the item from a catalogue, knowing that it will fit the client.
Currently the BHTA is working with Scottish procurement to help them to reduce the number of lots in their next Walking Aids tender. One of my aims with this will be hopefully to allow tenderers just to indicate the size (height, width, etc) range of each model they offer, and get away from terminology such as ‘narrow’ vs ‘hospital’, ‘children’ vs ‘adult’ vs ‘bariatric’, etc.
Conclusion
Where does that bring us? Maybe it’s best to use the term ‘children’ (in relation to equipment) to cover provision for young people going through rapid rates of change of internal and external development, where the assessment, adjustment, and replacement is going to be ongoing, and appropriate for where that person has reached along the road to stabilisation of their own respective development pathways. Bear in mind that physical, mental, and emotional development are unlikely to reach maturity at the same time (and even so, ultimately many of us return to ‘second childhood’, as our brains and bodies start to regress).
References
- https://lawstuff.org.uk/at-what-age-can-i/at-what-age- timeline/
- BS 8625:2019 Selection, placement and fixation of flexible postural support devices in seating. Specification