Categories
Speciality Areas
What makes a good cushion? Part 4: Contours for posture and positioning

This is the fourth article in a series which aims to start getting people thinking more about what goes into a cushion that makes it ‘good’ for one person, but maybe not for another.
In the first article we identified the three key elements around which a cushion can be assessed – functionality, posture management, and tissue integrity. In the third article we addressed the benefits of a neutral pelvis and stability for posture management. This article unpicks further aspects around posture and positioning that can be enhanced by selective contouring.
For the clinician, as well as for the occupant, tissue integrity around the buttocks may well come first when selecting the attributes of a cushion. As discussed in Part 3 of this series, the construction and resultant stability of the elements of the cushion’s design will have major effects – on the occupant’s ability to carry out their normal activities while on the cushion, on the one hand, and, on the other, effects on the control of deformities or preventing development of deformities elsewhere in the body.
In this article we consider further elements that can be incorporated into the design of a cushion through contouring to provide further postural support to the benefit of the occupant. Some of these elements, as well as helping the occupant to obtain the benefits of a better posture, will have a positive influence on pressure distribution.
Contouring
Contouring or shaping in cushions can be achieved by fixed components built into the cushion (e.g. different density or thickness of materials), by adjustability within the cushion (e.g. by selective removal of air), or by external additions (e.g. with shaped wedges under the cushion). This contouring or shaping can be placed selectively and to different degrees to meet the specific needs of the occupant. An alternative means of controlling posture and position, when contouring in or around the cushion is not enough, the application of positioning belts and harnesses, and appropriately placed pads may also be needed – either as a last resort, ideally.
Thus contouring can be designed to achieve specific aims to manage the occupant’s posture and positioning, which may lead to improved functionality and/or better controlled skeletal management, especially during growth phases. The downside is that contouring, by restricting some movement, may also have a negative outcome on functionality. In addition, the contours might physically impair transfers.
Thigh abduction
Anatomically, the ideal angle of the thighs is 5o of abduction from the midline, to ensure you have the head of the femur best located in the hip joint (the acetabulum) in the pelvis (Fig 1). This can be achieved by a thigh recess (trough) in the cushion, and/or extra or more dense material at the front of the cushion, creating an abduction pad between the thighs. These elements can also be used to help manage rotation of the pelvis. In more complex cases involving pelvic rotation and/or ‘windsweeping’, then the thigh recesses may need appropriate customisation.

Figure 1 Optimal thigh angles for femur-hip joint positioning
Lateral support
In contrast with the needs to adduct the thighs by a small amount, there will be times where there is a need to restrict the amount that the thighs abduct. This can be achieved by increased support built into the sides of the cushion – again by using more dense or additional material.
Sub-trochanteral support
A more specialist piece of posterior lateral support can be to create a ‘sub-trochanteral’ ledge. The greater trochanter is the boney prominence sticking out of the side of the femur near where it is located in the acetabulum. If the cushion has sufficient thickness (>10cm), and allows for sufficient immersion in the buttocks area, then some of the pressure from the ischial tuberosities can be ‘offloaded’ onto the greater trochanters, by the use of a sub-trochanteral ledge at the side of the cushion. By taking some of the body mass load onto this area, this also provides greater stability for the occupant, since the support base is at its widest at this point (Fig 2).
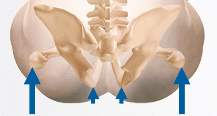
Figure 2. Greater trochanter offloading options
Please do be careful though: too much ‘offloading’ can have an adverse effect on the hip joint.
Obliquity management
In part 3 of this series, we referred to the pelvis as being like a basketball, which can rotate in all three planes. In that part we covered managing the ball’s tendency to roll backwards. Earlier in this article we’ve referenced any tendencies to rotate in the horizontal axis as seen from above from the transverse view. The third direction of possible rotation is seen when viewed from in front – a rotation we refer to as pelvic obliquity, where one side of the pelvis ends up higher than the other.
The degree of obliquity is measured by taking a line through the two ASISs at the front of the pelvis, and measuring by how many degrees this line deviates from the horizontal. If the right side is lower than the left this is a positive angle, but if higher then this is a negative angle1.

Figure 3. The association of pelvic obliquity with scoliosis of the spine
A pelvic obliquity is usually accompanied by a scoliosis of the spine, as the body tries to keep the head straight and the eyes horizontal (Fig. 3). The pelvic obliquity may be the cause of the scoliosis, or vice versa. Depending on the degree of flexibility of the spine, the shaping of the cushion may be used to accommodate the deformity, or assist in correcting it. To achieve this, sometimes it works better to decrease the thickness of the cushion on one side, and in other cases to increase the thickness. Using a pressure mapping device gives objective feedback as to the effectiveness of the respective interventions. The application of an appropriately placed positioning belt (often a rear pull one) can help in correcting a flexible obliquity2.
Gluteal (posterior) support
Apart from the ischial tuberosities under the pelvis, a major boney area at risk of pressure and shear injuries, is the sacral/coccyx area at the base of the spine – an area that has little skin protection, and an area that has forces from the back support as positions are changed.
any of us have more tissue than we feel we need around our buttocks. If we can spread the support of the body more widely over this area, we are taking the forces into tissues well away from inadequately covered boney prominences, as described in the paragraph above. Using a pressure mapping system which shows gradients as well as pressures can show clearly the potentially damaging forces around areas which are normally out of sight to the naked eye (Fig. 4).

Where the maximum pressures occur are not where the largest rates of change occur, and the greater the rate of pressure change, the greater likelihood of damaging shear strain. To what extent does your cushion provide contouring around this area (one area of contouring that, incidentally, will not have an adverse effect on transfers)?
Adding contours to a cushion

Adding, for example, a VariliteTM Contoured Positioning Wave Base (CPB) under a cushion, such as a RohoTM cushion, can provide additional support medially, laterally, and posteriorly.
In conclusion
There are many elements that should be taken into account when selecting what might be the most suitable cushion for an individual that go well beyond the immediate clinical needs of tissue integrity and the occupant’s needs for functionality. This article provides a number of the relevant related aspects that can be achieved through contouring of the cushion that can lead to a better posture, better function, and have tissue integrity benefits.
References
- WAUGH, K. and CRANE, B. A clinical application guide to standardized wheelchair seating measures of the body and seating support surfaces. Revised edition. Denver, CO: University of Colorado Denver, 2013. Available from: www.assistivetechnologypartners.org
- BS 8625:2019 Selection, placement and fixation of flexible postural support devices in seating – Specification (NOTE: Advice on the use and application of this standard is available from BES Healthcare Ltd.)